I. Peripheral arterial disease (PAD) or peripheral vascular disease (PVD)
Definition of PAD
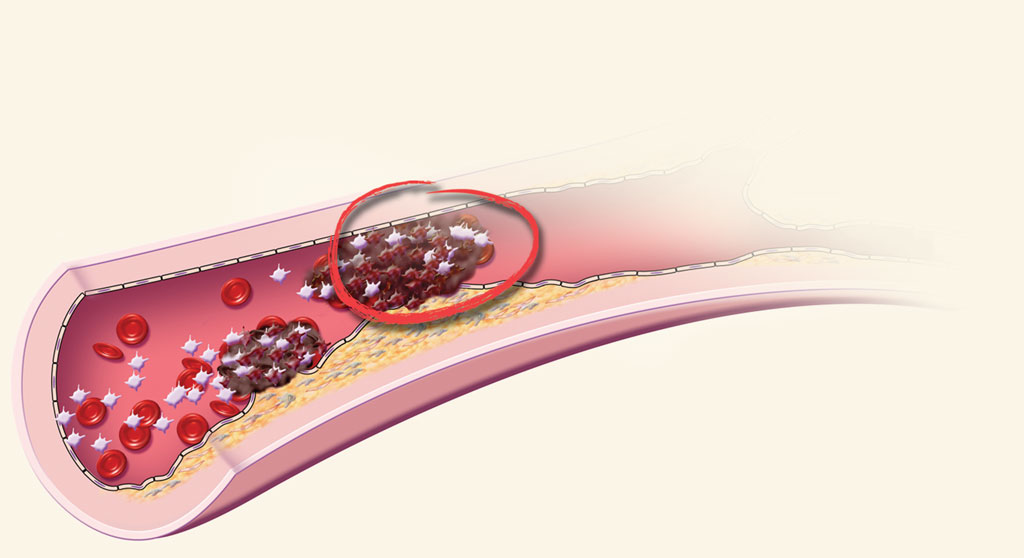
Peripheral arterial disease (PAD) is defined as a partial or total blockage of the arteries peripheral to the aorta. This is explained by an accumulation of lipids in the artery wall, called atherosclerosis. PAD evolves differently over time in patients. Many factors can modulate disease progression, such as the arterial site involved, personal and family medical histories and lifestyle habits.
Signs and symptoms of PAD can appear fairly late in life. For many, signs and symptoms will not appear until the artery is 60% narrowed or more. According to Statistics Canada (2015), almost 3 million Canadians, aged 50 to 79 years, have PAD. In response to arterial narrowing, adaptive mechanisms stimulate the formation of a network of small peripheral arteries that allow the blood flow to bypass the narrowed area and supply muscles and other body tissues which are further away, peripheral. This adaptive process is known as collateral blood supply and explains why some individuals may have PAD but experience few or no symptoms.
When a piece of cholesterol suddenly breaks off an arterial wall or a narrowed artery is blocked completely, blood flow will be totally obstructed, and the organ supplied by this artery will be damaged. The parts of the body most often affected by PAD are the legs.
- Worsening of PAD
The scope of the PAD problem depends on when it is diagnosed and pre-existing risk factors. The most important factors include smoking, high cholesterol, heart disease and diabetes (see Risk Factors section). In the final stages of PAD, circulation in the legs may be so poor that pain occurs in the feet and toes during periods of physical inactivity, such as during the night.
- Critical limb ischemia
The most advanced stages of PAD can lead to critical limb ischemia (CLI). In CLI, severe arterial obstruction is detected, which seriously decreases blood flow to the extremities (hands, feet and legs). This situation can degenerate into intense pain and even cause skin ulcers or wounds since they do not receive the oxygen-rich blood necessary for tissue growth and repair. In some cases, gangrene (tissue death) may set in. This condition, if untreated, may lead to amputation.
Symptoms of PAD
In its least severe form, PAD is silent and does not cause any symptoms; it can only be detected by diagnostic exams. Symptoms experienced with physical effort should be discussed with your doctor. For many, the first symptom to appear is a painful leg muscle cramp when walking, which consequently leads to intermittent claudication. Rest is the only action which will make the cramping go away. This leg pain may be serious enough to discourage a person from walking normally. Other people experience no cramps or pain, but they will feel numbness, weakness or heaviness in the muscles.
- Other symptoms

In patients whose PAD is more severe, insufficient blood flow to the feet and legs can cause sharp, burning pain in the feet and toes at rest. The pain occurs particularly at night when lying down.
There are other symptoms to watch for:
- Cold skin in specific areas of the legs or feet
- Changes in skin colour and loss of hair
- Wounds on the toes and feet that do not heal
- Silent PAD
Many people have PAD but are asymptomatic. These people are at high risk of having a heart attack or stroke. Recently, it has been shown that the life expectancy of people with PAD is considerably shorter. For example, the risk of dying of heart disease is six times higher in people with PAD that in people who do not have it. Therefore, it is important to discuss this disease with a healthcare professional if you have the symptoms listed above or risk factors for PAD.
Preventing PAD
The most important part of PAD is continuing to exercise as tolerated. Walking until symptoms occur causes muscles to function better and helps promote better circulation. Physical activity, such as walking, is beneficial for cardiovascular health and affects all the risk factors associated with developing PAD.
It is also important to control some of the preventable or curable risk factors:
- Quit smoking
This is the “number 1” risk factor for developing PAD. Nicotine and the other agents in cigarettes contribute to the development of atherosclerosis which is responsible for narrowing of the arteries, leaving less room for blood flow. Smokers are not only at risk of developing arterial disease, but also interfering with treatment attempts.
- If overweight, lose weight
Secondly, managing cholesterol by changing eating habits and taking drugs such as statins is important. By lowering cholesterol levels, you can delay or even reverse plaque buildup in the arteries. The Heart and Stroke Foundation offers information on their website related to questions about cholesterol, risk factors associated with hypercholesterolemia, dietary recommendations and therapeutic interventions available.
If you have diabetes, it is important to see your doctor often to ensure optimum control of blood glucose levels and prevent the onset of problems with vision, nerves, heart, kidneys and peripheral vessels. Lastly, appropriate, frequent foot care is also strongly recommended for diabetic patients.
- Limiting salt intake
It is estimated that one person in three is sensitive to sodium, which is found in salt. This means that excess sodium consumed by those people may increase the fluid volume circulating in their arteries, and at the same time contribute to raising their blood pressure. In the long-term, high blood pressure becomes a major risk factor for developing a stroke, heart disease and kidney disease. Therefore, decreasing your daily salt intake contributes to reducing blood pressure and indirectly to protecting the organs listed above.
75% of patients with PAD are asymptomatic, so doctors need to be pro-active and vigilant with patients at risk of this disease. Appropriate diagnostic tools are a comprehensive questionnaire, a vascular physical examination including a measure of the ankle-brachial index, Doppler ultrasound and/or magnetic resonance angiography (MRA)..
It is important to provide enough information about your symptoms to your doctor to enable classification of the severity of the PAD and inform a prescribed treatment based on the clinical stage of the disease within an appropriate period of time.
Medical and non-surgical management of PAD
All patients with atherosclerosis should take certain medicines to prevent progression of their disease, including patients with PAD. These drugs prevent the disease from developing, and therefore decrease the chances of having vascular complications:
- Aspirin or other anti-platelet agent
- A statin to reduce LDL-cholesterol
- And check with your doctor for other drugs that are under development.
- Treatment options

Treatment options vary and depend on a patient’s overall health and the severity of the diagnosis. Physicians need to provide patients with adequate information to help understand all the options. Many patients with PAD and intermittent claudication are treated without surgery. Long-term studies on large numbers of patients with intermittent claudication have demonstrated that only 25% of them had worsening symptoms.
A preventive treatment plan for PAD involves the following elements:
- Adopting a Mediterranean-style diet low in saturated fat (rich in fruits and vegetables, whole grain products, legumes, nuts and olive oil) helps to prevent buildup of atherosclerotic plaque.
- Starting aerobic physical exercises is also an important preventive measure.
- If you are a smoker, quitting smoking has a major impact on disease development.
In six months you will begin to see the effects of your doctor’s recommendations. However, the benefits last only as long as you continue with the changes made. If you start smoking again, for example, you will end up where you began. You will need to see your changes as a new way of life.
In addition, a therapeutic exercise program focused on aerobic exercise can be beneficial for everybody. This means a prescription for individualized exercise designed to restore vascular health and prevent disease progression. The prescription is written by a doctor, in collaboration with a kinesiologist. This healthcare professional considers your current state of health and provides advice about the type of exercise to do, intensity, duration and frequency of workouts.
Surgical treatment of PAD
There are many types of very effective procedures that can help improve circulation, increase walking distance, heal foot ulcers and prevent amputation.
The Canadian Society for Vascular Surgery suggests that all patients with critical ischemia should have surgery to prevent gangrene and amputation. This applies to all patients with resting pain in the leg or foot associated with PAD. In addition, patients with ulcers or gangrene associated with PAD are candidates for surgery.
Family doctors, internists or other Internal Medicine subspecialists can direct patients to a vascular surgeon or interventional radiologist as needed.
Patients with intermittent claudication, only during physical exercise, run no risk of amputation. Surgery should be considered only if their symptoms become debilitating, i.e., significantly limiting physical activity associated with daily living.